Cornea
is one of the most important and sensitive parts of the human eye as it
contributes the majority of its refractive power and also provides a clear
entrance to the light rays in the eye.1 Cornea is privileged because
of its transparency which depends mainly upon its avascularity,2
dehydrated state, smooth surface epithelium and well organized stromal collagen
fibers.3 Although cornea does not depend on oxygen provided by lungs
through blood and takes oxygen from air directly,4 but this a vascularity
makes it vulnerable to a variety of infections because it is deprived of the
usual defense mechanisms of the body in the form of circulating polymorphs,
lymphocytes and antibodies. Although there is some protection for the cornea in
the form of lysozyme, lactoferrin, IgA, lipocalin5
etc, but it is meager and the cornea acts like a tied prisoner in the face of
pathogens when it is breached. Infectious keratitis is the most common cause of
uniocular blindness in the world6. In
Pakistan corneal opacity is the second most common cause of blindness after
cataract.7 Infectious or microbial keratitis can be caused by a wide
spectrum of organisms, including a huge variety of bacteria, fungi, viruses and
parasites.8 A lot of variation is seen in the etiology and
epidemiology of infectious keratitis from place to place9 and time
to time, that’s why it is essential to have local data available, so that the
burden of problem is understood and preventive and curative strategies are
planned and established. The objective of this study was to identify the
different causes of infectious keratitis and their prevalence and frequencies
in the patients coming to the Department of Ophthalmology, Chandka Medical
College and Hospital Larkana. MATERIALS AND METHODS This was a prospective case series study
carried out at the Department of Ophthalmology, Chandka Medical College
Hospital Larkana, Sindh, Pakistan, from February 2004 up till February 2015.
All patients attending the outpatient department, clinically diagnosed as a
case of infectious keratitis and given informed consent were included in the
study. Patients excluded from the study were under the age of 16 years, or
having Mooren’s ulcer, or ulcers associated with
exposure, autoimmune and systemic diseases. Corneal swabs or scrapings were
taken and the specimens were prepared on three separate slides, one was
prepared with potassium hydroxide (KOH 10%) to see the fungal hyphae or pseudohyphae, the second stained with Gram’s stain to
identify the bacteria, and the third was stained with hematoxylin
and eosin stain to look for Acanthamoeba. Slides were
then seen under the microscope for evaluation and final report. A standard
proforma was filled for each patient, which included
gender and age of the patient, clinical diagnosis and the results of corneal
scrapings except for the patients suspected of viral ulcers, in which case the
diagnosis was clinical and considered definite if there was improvement seen on
antiviral treatment. In case of polymicrobial
infections if Acanthamoebae were identified then it
was labeled as Acanthamoeba keratitis regardless of
the results of the other two slides. If fungal hyphae were seen, it was labeled
as fungal keratitis. Bacterial keratitis was only labeled if bacteria alone
were seen. SPSS version 20 was used for data entry and analysis.
RESULTS
A total
of 2411 patients were clinically diagnosed as having infectious keratitis and
included in the study during the period of eleven years, out of which 1447
(60.02%) were males and 964 (39.98%) were females (Fig. 1). The mean age (±
standard deviation) was 36.73 ± 15.49 years and the range was 17 – 76 years.
The final report after combining the results of corneal scrapings and clinical
diagnosis showed that 1353 (56.12%) patients were fulfilling the criteria of
bacterial keratitis. 927 (38.45%) patients had fungal keratitis, 88 (3.65%)
patients were diagnosed as case of viral keratitis and 43 (1.78%) patients had Acanthamoeba keratitis (Fig. 2). DISCUSSION This study shows that males have a greater tendency to
fall prey to infectious keratitis than females, which is consistent with other
studies from Pakistan,8,12 Malaysia24
and India.20 This is probably due to greater
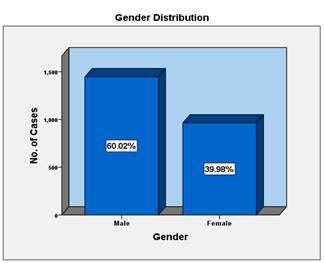
Fig. 1:
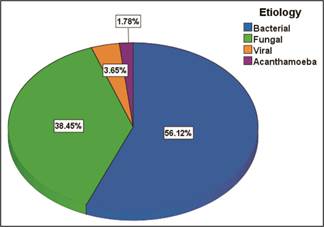
Fig. 2:
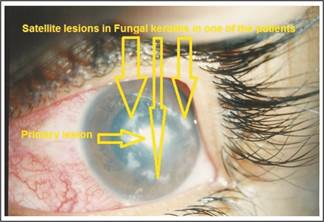
Fig. 3: Fungal keratitis.
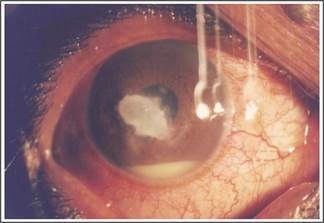
Fig. 4: Bacterial keratitis
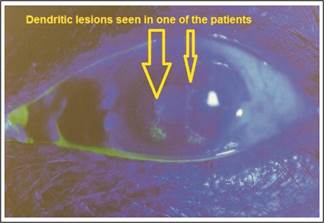
Fig. 5:
Viral
keratitis (Herpes simplex)
exposure of males to outdoor risk factors, physical activity and professional
hazards. Patients in middle ages are more prone to develop infectious keratitis
according to our study, which is similar to the studies from Pakistan8,12 and India20. The mean age being 36.73 ±
15.49 years which is lower than the mean age
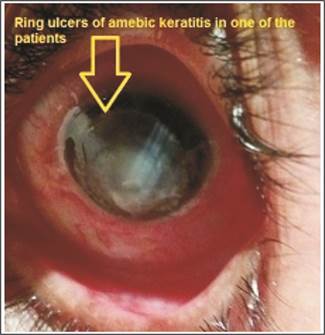
Fig. 6:
Amebic keratitis.
(44.5 ± 20.9 years) reported by Norina TJ et al24 and
the mean age (64.3 ± 10.3 years) reported by Ahn M
et al22. This study shows that bacteria are more common
(56.12%) among the organisms causing infectious keratitis and it is consistent
with some other research studies around the world8, 10, 11,
although, other studies have reported fungus as the major cause of infectious
keratitis.12-15 Epidemiology of infectious keratitis varies with
geography and climate but generally Gram-positive bacteria are more frequently
recovered in temperate climatic regions16-18 and Gram negative
bacteria and fungi in tropical or sub-tropical climates19, 20.
Stapleton F et al21 states that Fungi
account for 5 – 40% of culture proven infections which is rather similar to our
results of 38.45%. In our study the cases of viral keratitis were 3.65% less
than that reported by Patel S et al23 and that of Acanthamoeba keratitis (1.78%) were approximately equal to
that reported by Srinivasan M et al25 (1%) and less than that
reported by Riaz Q et al12 (8%).
CONCLUSION
Infectious keratitis is an economic and social
problem of huge magnitude due to the fact that the affected population is
middle aged, males more than females who are actively involved in their household
and national progress. Bacteria and Fungi are responsible for the bulk (94.57%)
of infectious keratitis but Virus and Acanthamoeba
may not be underestimated.
Author’s
Affiliation
Dr Syed Imtiaz Ali Shah
Professor
Department of Ophthalmology
Chandka Medical College Larkana
Dr. Shujaat Ali Shah
Trainee Registrar
Department of Ophthalmology
Chandka Medical College Larkana
Dr. Partab Rai
Professor
Department of Ophthalmology
Chandka Medical College Larkana
Dr. Safdar Ali Abbasi
Ophthalmologist
Department of Ophthalmology
Chandka Medical College Larkana
Dr. Huda Fatima
Trainee Registrar
Department of Ophthalmology
Chandka Medical College Larkana
Dr. Ali Akbar Soomro
Professor
Department of Pathology
Chandka Medical College Larkana
Role of
Authors
Dr Syed Imtiaz Ali Shah
Manuscript writing, study design.
Dr. Shujaat Ali Shah
Data analysis, review of images.
Dr. Partab Rai
Manuscript review.
Dr. Safdar Ali Abbasi
Manuscript review.
Dr. Huda Fatima
Manuscript design.
Dr. Ali Akbar Soomro
Manuscript writing.
REFERENCES
1.
Willoughby CE, Ponzin D, Ferrari S, Lobo
A, Landau K, Omidi Y. Anatomy and physiology of
the human eye: effects of mucopolysaccharidoses
disease on structure and function–a review. Clin Exp Ophthalmol. 2010; 38: 2-11.
2.
Azar DT. Corneal angiogenic privilege: angiogenic and antiangiogenic
factors in corneal avascularity, vasculogenesis,
and wound healing (an american
ophthalmological society thesis). Trans
Am Ophthalmol Soc. 2006; 104: 264-302.
3.
Qazi Y,
Wong G, Monson B, Stringham J, Ambati
BK. Corneal transparency: genesis,
maintenance and dysfunction. Brain Res
Bull. 2010; 81: 198-210.
4.
Leung BK, Bonanno JA, Radke CJ.
Oxygen-deficient metabolism and corneal edema. Prog Retin Eye Res. 2011; 30: 471-92.
5.
McDermott AM. Antimicrobial
Compounds in Tears. Exp Eye Res.
2013; 117: 53-61.
6.
Tananuvat N, Suwanniponth M. Microbial Keratitis in Thailand: a survey of common practice
patterns. J Med Assoc Thai. 2008; 91: 316-22.
7.
Dineen B,
Bourne RR, Jadoon Z, Shah SP, Khan MA, Foster A et
al. Pakistan National Eye Survey
Study Group. Causes of blindness and visual impairment in Pakistan. The Pakistan national blindness and visual impairment survey. Br J Ophthalmol. 2007; 91: 1005-10.
8.
Sethi S, Sethi MJ, Iqbal R. Causes of microbial keratitis in patients attending an eye clinic
at Peshawar. Gomal J Med Sci. 2010; 8: 20-2.
9.
Shah A, Sachdev A, Coggon D, Hossain P.
Geographic variations in microbial keratitis: An analysis of the Peer-Reviewed
Literature. Br J Ophthalmol.
2011; 95: 762-7.
10.
Tewari A, Sood N, Vegad MM, Mehta DC. Epidemiological and microbiological profile of infective keratitis
in Ahmedabad. Ind J Ophthalmol.
2012; 60: 267-72.
11.
Al-Shakarchi FI. Initial therapy for suppurative
microbial keratitis in Iraq. Br J. Ophthalmol. 2007;
91: 1583-7.
12. Riaz Q, Fawwad U, Bhatti
N, Rehman A, Hasan M. Epidemiology of microbial keratitis in a
tertiary care center in Karachi. Pak J Ophthalmol. 2013;
29: 94-9.
13.
Hitesh J Assudani, J M Pandya, R R Sarvan,
A M Sapre, A R Gupta, S J
Mehta. Etiological diagnosis of
microbial keratitis in a tertiary care hospital in Gujarat. Natl
J Med Res. 2013; 3: 60-2.
14.
Lin CC, Prajna L, Srinivasan
M, Prajna VN, McLeod SD, Acharya
NR Lietman TM, Porco TC. Seasonal Trends of Microbial Keratitis in South India. Cornea. 2012; 31: 1123-7.
15.
Leck AK,
Thomas PA, Hagan M, Kaliamurthy J, Ackuaku E, John M Newman MJ,
Codjoe FS, Opintan JA, Kalavathy CM, Essuman V, Jesudasan CA, Johnson GJ.
Aetiology of suppurative corneal ulcers in Ghana
and south India, and epidemiology of fungal keratitis. Br J Ophthalmol. 2002; 86: 1211-5.
16.
Bourcier T,
Thomas F, Borderie V, Chaumeil
C, Laroche L. Bacterial keratitis: predisposing factors, clinical and
microbiological review of 300 cases. Br J Ophthalmol. 2003; 87: 834-8.
17.
Keay L,
Edwards K, Naduvilath T, Taylor HR, Snibson GR, Forde K Stapleton F. Microbial keratitis: predisposing factors and morbidity.
Ophthalmology. 2006; 113: 109-16.
18.
Bennett HG, Hay J, Devonshire P, Seal DV, Kirkness
CM. Antimicrobial treatment of
presumed microbial keratitis: guidelines for treatment of central and
peripheral ulcers. Br J Ophthalmol. 1998; 137-45.
19.
Fong CF, Tseng CH, Hu FR, Wang IJ, Chen WL, Hou
YC. Clinical characteristics of
microbial keratitis in a university hospital in Taiwan. Am J Ophthalmol. 2004; 137: 329-36.
20.
Gopinathan U,
Sharma S, Garg P, Rao GN. Review of epidemiological features, microbiological diagnosis and
treatment outcome of microbial keratitis. Ind J Ophthalmol. 2009; 57: 273-9.
21.
Stapleton F, Carnt N. Contact lens – related microbial
keratitis: how have epidemiology and genetics helped us with pathogenesis and prophylaxis. Eye,
2012; 26: 185-93.
22. Ahn M,
Yoon KC, Ryu SK, Cho NC, You IC. Clinical aspects and
prognosis of mixed microbial (bacterial and fungal) keratitis. Cornea. 2011; 30: 409-13.
23.
Patel S, Chaudhari AM, Solu TM, Gharat V. Epidemiological and Microbiological profile of patients having
Microbial Keratitis. Natl J Community Med. 2014; 5:
463-7.
24.
Norina TJ, Raihan S, Bakiah S, Ezaqnee M, Liza SAT, Wan HWH. Microbial Keratitis: aetiological
diagnosis and clinical features in patients admitted to Hospital Universiti Sains Malaysia.
Singapore Med J. 2008; 49: 67-71.
25.
Srinivasan
M, Gonzales CA, George C, Cevallos V, Mascarenhas JM, Asokan B Wilkins J,
Smolin G, Whitcher JP. Epidemiology and etiological diagnosis of corneal ulceration in
Madurai, South India. Br J Ophthalmol. 1997; 81:
965-71.